










Imagine taking a bite of your favorite meal, only to feel it “stuck” halfway down your chest, no pain at first, just that frustrating sensation that something isn’t moving. For thousands of Americans living with Achalasia, this is daily life. Once called “cardiospasm,” achalasia is a rare but treatable swallowing disorder affecting roughly 18 out of every 100,000 people in the U.S., with incidence nearly doubling between 2014 and 2024.
It strikes adults most often between ages 30 and 60, though it can appear at any age. The good news? While there’s no cure yet, modern treatments like POEM and Heller myotomy can restore comfortable eating for most people, helping you reclaim meals, energy, and peace of mind. In this guide, we break down everything, from what happens inside your body to practical daily tips, so you or a loved one can navigate achalasia with confidence.
What is Achalasia?
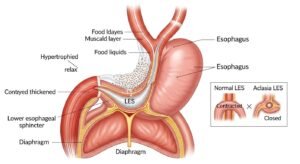
Achalasia is a motility disorder of the esophagus, the muscular tube that carries food and liquids from your mouth to your stomach. In a healthy esophagus, coordinated wave-like contractions (called peristalsis) push food downward. At the same time, the lower esophageal sphincter (LES), a ring of muscle at the bottom, relaxes to let everything pass into the stomach.
With achalasia, those waves disappear, and the LES stays tightly closed. Food and liquid back up like water behind a dam, leading to regurgitation, chest pressure, and difficulty swallowing. It’s not cancer, reflux, or a simple blockage; it’s a nerve-and-muscle communication problem. Affecting about 1-2 new cases per 100,000 people each year in the U.S., it’s uncommon but increasingly recognized thanks to improved diagnostic tools.
Symptoms and Causes
The most common symptom is dysphagia, trouble swallowing both solids and liquids, which feels like food is stuck in your chest or throat. Many people also experience:
- Regurgitation of undigested food or saliva (often at night)
- Chest pain or spasms that mimic heartburn
- Unexplained weight loss
- Coughing or choking while eating
- Frequent heartburn-like sensations or a lump-in-throat feeling
Symptoms usually develop gradually over months or years, so they’re often mistaken for GERD, anxiety, or even eating disorders.
Causes remain unclear, but the leading theory points to an autoimmune process: your immune system mistakenly attacks the nerve cells (myenteric plexus) in the esophagus, often triggered by a prior viral infection. Genetic factors can increase risk (especially rare syndromes like Allgrove), and some people have family links or co-existing autoimmune conditions such as rheumatoid arthritis or Sjögren’s. It is not contagious or caused by lifestyle alone.
Types of Achalasia
High-resolution manometry divides achalasia into three main subtypes based on how the esophagus behaves, crucial for choosing the best treatment:
- Type I (Classic): No peristalsis and a completely relaxed LES pressure pattern. Food simply sits; good response to most treatments.
- Type II (Most Common and Best Prognosis): Pressurized “panesophageal” contractions. Responds exceptionally well to balloon dilation or POEM (up to 90-95% success).
- Type III (Spastic): Premature or spastic contractions causing severe chest pain. Often needs POEM for the highest success rate.
Your subtype is determined during diagnosis and directly guides whether medications, dilation, or surgery will work best.
Diagnosis and Tests
Because symptoms overlap with other conditions, accurate diagnosis is key. Doctors typically start with:
- Barium swallow (esophagram): You drink a chalky liquid while X-rays show the classic “bird-beak” narrowing at the stomach entrance.
- High-resolution esophageal manometry: The gold-standard test: a thin tube measures muscle contractions and LES pressure during swallows. It also confirms your subtype.
- Upper endoscopy: A camera rules out tumors or pseudoachalasia (cancer mimicking achalasia).
- Sometimes,s pH monitoring or CT scans are needed.
Early diagnosis prevents malnutrition and lung complications from repeated aspiration.
Management and Treatment
There is no cure, but treatments focus on relaxing or opening the LES so food can pass. Options range from temporary fixes to long-lasting procedures:
- Pneumatic balloon dilation (outpatient, stretches the sphincter)
- Peroral endoscopic myotomy (POEM), a scarless, minimally invasive procedure that cuts the muscle from inside the esophagus, is now the preferred option in many U.S. centers, with 90%+ success.
- Heller myotomy (laparoscopic surgery) plus anti-reflux wrap
- Botox injections (temporary bridge for older or frail patients)
Success rates are high, but some people need repeat procedures years later. Your gastroenterologist will tailor the choice to your subtype, age, and overall health.
Medications for Achalasia
Medications offer only short-term relief and are rarely used alone:
- Calcium channel blockers (e.g., nifedipine) or nitrates relax the LES temporarily.
- They help mild cases or while awaiting a procedure, but lose effectiveness over time and can cause side effects like headaches or low blood pressure.
They’re most useful as a bridge, not a long-term plan.
Botulinum Toxin Injections
Botox (botulinum toxin) is injected directly into the LES during endoscopy. It blocks the nerve signals that keep the sphincter tight, providing relief for 3-6 months (sometimes up to a year). It’s quick, low-risk, and ideal for elderly patients or those who aren’t surgical candidates. Many use it while deciding on POEM or myotomy. Repeat injections are possible but become less effective over time.
What Happens to Muscles with Achalasia
Here’s the science in plain terms: Your esophagus relies on two types of nerves, excitatory (squeeze) and inhibitory (relax). In achalasia, the inhibitory nerves (which release nitric oxide and VIP to calm the muscle) are destroyed.
Without them, the LES stays contracted, and the esophageal body loses its wave-like peristalsis. Over time, the esophagus may dilate (megaesophagus in severe cases), food ferments, and pressure builds. This explains the backup, regurgitation, and chest pain.
Outlook / Prognosis
With proper treatment, most people with achalasia enjoy a normal life expectancy and good quality of life. Untreated, risks include severe malnutrition, aspiration pneumonia, and a slightly higher chance of esophageal cancer (still rare).
Post-treatment, some develop reflux that’s easily managed with acid reducers. Regular follow-up keeps complications low, and many patients eat normally again within weeks.
Living With Achalasia
Daily life improves dramatically once you adapt:
- Eat slowly in an upright position; stay upright 30-60 minutes after meals.
- Take small bites, chew thoroughly, and sip water between bites.
- Elevate the head of your bed 6-8 inches to reduce nighttime regurgitation.
- Avoid carbonated drinks, very cold or very hot foods, and tough textures at first.
- Keep a food diary to identify personal triggers.
Join U.S. support groups (like Achalasia Awareness or Facebook communities) for practical tips and emotional support. Many patients say connecting with others is life-changing.
Best Care of Achalasia
Best care means a multidisciplinary team: a gastroenterologist experienced in motility disorders, a surgeon skilled in POEM or Heller, and a registered dietitian. Get care at high-volume esophageal centers (many top U.S. hospitals now list them). Track symptoms with the Eckardt score (a simple 0-12 scale) and schedule follow-up manometry if symptoms return. Early intervention prevents long-term damage.
FAQs
Is Achalasia an autoimmune disease?
Yes, it is widely considered an autoimmune or immune-mediated condition. The body appears to attack its own esophageal nerve cells, often after a viral trigger. Many patients also have other autoimmune disorders.
When Should You See a Doctor for Achalasia Symptoms?
See a doctor promptly if you have persistent difficulty swallowing solids and liquids, frequent regurgitation, unexplained weight loss, or chest pain with eating. Don’t wait; early diagnosis dramatically improves outcomes.
Is there a genetic link?
There is a genetic predisposition in some families, and rare inherited syndromes (like Allgrove) cause achalasia. Most cases, however, are not directly inherited but may involve genetic factors that make certain people more susceptible to autoimmune nerve damage.
Is achalasia deadly?
No. With treatment, it is not life-threatening. Untreated severe cases can lead to dangerous complications like aspiration pneumonia or extreme malnutrition, but these are preventable.
Is there an achalasia diet?
Yes, focus on soft, moist, calorie-dense foods: smoothies, mashed potatoes, yogurt, scrambled eggs, well-cooked pasta, and puréed soups. Chew thoroughly, eat small, frequent meals, and avoid dry meats, bread, raw vegetables, and carbonated beverages. A dietitian can create a personalized plan to prevent weight loss while keeping meals enjoyable.
Conclusion
Achalasia may feel overwhelming at first, but you’re far from alone and far from helpless. With today’s precise diagnostics and highly effective treatments like POEM, most people regain the joy of eating without fear. Listen to your body, work with experienced specialists, and lean on the growing community of patients who are thriving.
If you suspect achalasia, reach out to a motility expert soon. Knowledge and the right care can turn “stuck” into “smooth sailing” again. Share this guide, ask questions in the comments, and take that first step toward feeling better. You’ve got this.



